Health literacy is essential for containing and solving global health crises such as COVID-19. By contrast, scientifically unconfirmed and false data can be shared quickly, fomenting fear and collective resistance to existing and potential medical solutions. To counter the rising anti-science rhetoric and the lack of compliance with public health measures, we propose a Global Health Literacy Alliance that will bolster collective capacity to access and process scientific information. The ambition is to shift public knowledge and perception of health from Life Sciences, often cryptic and technical, into a broader, open, understandable and participative “Sciences for Life” culture.This brief discusses the potential of this initiative to ensure better informed pandemic (and further health crises) responses, promote equal access to healthcare services, strengthen societal resilience and boost sustainable growth and well-being.
Challenge
The interconnectedness of our global communities and individual compliance with different state-mandated orders have emerged as crucial for the effectiveness of our global pandemic containment. COVID-19 has highlighted the role of scientific research especially related to health for collective well-being, health, safety and economies. Popular familiarity with accurate health information, scientific methods and the innovative solutions developed is therefore becoming a determining factor of our communities’ ability to contain and prevent public health crises.
Limited popular understanding of science, scientific methods and processes confines scientific debates focused on health to academic circles alone, which leaves space for anti-scientific rhetoric. In turn, this creates barriers to innovations in Life Sciences and to individuals’ adherence to national and international recommendations.
First proposed in the 1970s (Simonds, 1974), health literacy (HL) is a set of skills or a hierarchy of functions: the ability to read and understand health information (functional), the cognitive and social skills that allow greater engagement with a wider variety of health information (interactive) and the higher cognitive and critical decision-making skills that are needed, alongside social, political and organizational action, in order to improve wider determinants of health (critical) (Nutbeam, 2000). Hence, HL impacts a person’s ability to access healthcare, to care for themselves and to elaborate upon and communicate health-related concepts with a view to protecting their health (Kickbusch, 2008).
HL has become an issues of increasing interest, as its benefits for individual and public health and also the sustainability of healthcare systems have been recognized (Nutbeam, 2000; Nielsen-Bohlman, Panzer and Kindig, 2004; Ishikawa and Yano, 2008; Peerson and Saunders, 2009; Berkman et al., 2011; Sørensen et al., 2012). It is considered to be particularly important in countering non-communicable diseases (NCDs) (Bezinger, Roth and Moran, 2016), highlighting the need for individuals to take more responsibility in managing their own health so that health services are used more effectively(Mcqueen, Kickbusch and Potvin, 2007; Kickbusch and Reddy, 2016; Fitzgerald et al., 2020).
Low HL is associated with difficulties in comprehending health information and scant knowledge about diseases and therapeutic adherence. This contributes to poor health, a higher risk of mortality, ineffective use of healthcare services, increased costs and health inequalities (Nielsen-Bohlman, Panzer and Kindig, 2004; Peerson and Saunders, 2009; Berkman et al., 2011). Several evidence-based studies have addressed HL as one of the most promising and cost-effective approaches to overcoming the challenges of communicable diseases and NCDs (Pleasant, 2014; Pleasant et al., 2015).
The COVID-19 pandemic has challenged global health, security and sustainable and equal growth, exacerbating inequalities and putting unprecedented pressure on healthcare systems and governments around the world. While the tackling of the root causes of these problems is an urgent task, promoting HL can contribute to strengthening the effectiveness of global health systems, minimizing social health inequity, mitigating the risk of protracted viral epidemics and preventing future health crises.
For these reasons, the EU, the USA, Canada, Australia and China, among others, have included HL as a key priority in their policies (Institute of Medicine, 2013). The World Health Organization (WHO) has also suggested HL as a prerequisite for several UN Sustainable Development Goals (SDGs) (WHO, 2017) in particular SDG 4 “Achieving inclusive and equitable access to education” and SDG 3 “Ensure healthy lives and promote well-being for all at all ages” both of which are being challenged by the pandemic. The Rome Declaration, which was drafted and signed by G20 leaders during the Global Health Summit (May 2021), further commits to supporting “the achievement of the SDG, their targets, and specific initiatives such as the Global Action Plan for Healthy Lives and Wellbeing for all to better support countries to accelerate progress towards the health-related SDG including towards Universal Health Coverage”.
Despite its importance, there are currently no systems for specifically measuring HL functional, interactive and critical for different ages (teens, adults and the elderly) at a global level. There are only broader scientific literacy maps that focus on cross-national comparisons, while research on stratification, variation, and disparities specific to HL is not available. This means that clear mapping of knowledge gaps on health around the world is lacking, which will ultimately hinder solutions to the current global health crises. Moreover, regional estimates show alarmingly poor levels of HL, even among healthcare personnel (Coleman et al., 2013; Msaouel et al., 2014). Unequal literacy rates clearly show a correlation with the growth of an anti-science movement (Hoopman et al., 2009; Kobetz et al., 2009; Nazri, 2019; Nichols and Petzold, 2021; Scherer et al., 2021; Solomon, 2021).
HL is inadequate on average in most EU countries, as shown by the findings from the first European comparative survey on HL in populations, which was conducted in eight EU countries (Austria, Bulgaria, Germany, Greece, Ireland, the Netherlands, Poland and Spain), based on Eurobarometer standards. At least one in ten respondents (12 per cent) showed insufficient HL and almost half (47%) had limited HL (Sørensen et al., 2015).
In sub-Saharan Africa, the situation is worse, with 64.8 per cent of the population (McClintock et al., 2017) unable to meet the basic comprehension benchmark. This region is already struggling to access vaccines, owing to unacceptable delays in supply and global inequality. Forestalling any anti-scientific impulses is therefore crucial in ensuring access to medication and overall youth engagement in public health solutions over the long term. According to OECD PISA score 2018, over 10 million students (fifteen-year-olds) were not able to complete even the most basic reading tasks, while one student in four had difficulty in connecting pieces of information provided by different sources and only one in ten was able to distinguish facts from opinions. Older people also show a poor level of HL, which correlates with less predilection for healthy behaviours (Do, 2020). Providing tools so that the importance of self-care can be understood is considered to be one of the main tools for counteracting health inequality.
Nevertheless, poor HL is still an underestimated public health issue globally (Zarocostas, 2020). Conveying accurate information is urgent and necessary, but it is not sufficient to induce changes in citizens’ beliefs and behaviours. We therefore need to offer shared tools that will allow scientific methods to be understood and will promote critical thinking that supports health innovation as well as social and economic growth. Improving HL should be considered as a tool that can tackle disintermediation between institutions and citizens. The European Parliament highlights for example that “scientific literacy can provide people with tools to navigate and critically address vast amounts of information exchanged in public debates, [and] support democratic processes”, thus forming responsible and active citizens in a democratic society (Siarova, Sternadel and Szőnyi, 2019). The same consideration should be given to HL, which can stimulate active citizens’ participation in public debate and in decisions related to healthcare systems, thereby enhancing their efficiency, sustainability and equality.
The challenge of HL is clear, but currently the lack of a shared and accurate measurement of its gaps at global level is still the main challenge. Ensuring clear standards of health in order to promote resilience and well-being, and to fight health inequalities and anti-scientific rhetoric requires clear commitments and measurable targets. Finally, international cooperation, mutual learning between institutions, companies, chief scientific officers (CSOs) and academia should be a strategic asset that is managed and promoted by a dedicated international organization; this currently does not exist.
Proposal
Under the auspices of the G20, the world’s most prominent political figures can turn this situation around. Timely interventions are essential since increasing rates of HL are needed to tackle inequality and enable access to and diffusion of scientific solutions. To this end, we propose a Global Health Literacy Alliance, under the umbrella of (or through enhanced cooperation between) the WHO and UNESCO. Considering that HL relies on a variety of sources of information, factors and stakeholders in our complex societies, the Alliance should involve the same wide representation in order to promote alignment and the orientation of coherent goals.
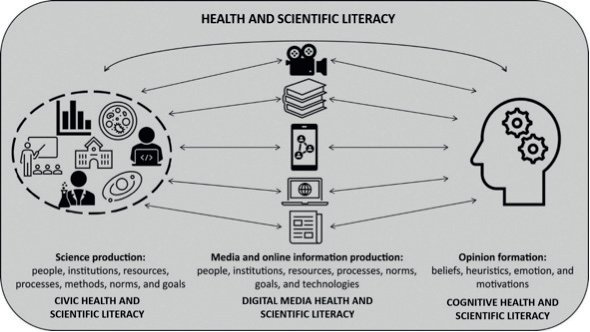
Figure 1. A representation of the dimensions of literacy that are necessary for scientific literacy, spanning the lifecycle of scientific information in society
Adapted from Howell and Brossard (2021)
Hence, the Alliance will be represented by diverse country delegates including youth, scientists, politicians and heads of agencies, academia, clinicians, neuro-cognitive experts, CSOs representatives and communication specialists.
This initiative will be open to collaborations with other actors, such as the World Bank, European Investment Bank, African Development Bank, Inter-American Development Bank, Asian Development Bank, European Commission, the Association of Southeast Asian Nations, the Organisation for Economic Co-operation and Development, the WHO, the United Nations Children’s Fund (UNICEF), the African Union, Scientific Innovation Labs, academic partners and other multilateral organizations.
We suggest four operational phases that the Alliance should focus on in order to respond to the challenges highlighted.
PHASE 1
Identifying and measuring the challenge: Global Health Literacy Map
The first Alliance challenge is to provide a tool similar to the OECD’s Financial Literacy initiative, outlined in the Russian’s G20 Presidency’s call to “promote the development of reliable data on the levels of financial literacy to support the designing phases of national strategies” (OECD, 2017).
Unlike scientific literacy, there are currently no systems for measuring different types of HL-functional, interactive and critical for different ages (teens, adults, and elderly) based on shared global criteria. This leads to a lack of clear mapping of knowledge gaps related to global health around the world, and this hinders the discovery of solutions.
HL embraces three key broad elements: (1) knowledge of health, healthcare and health systems; (2) processing and using information in various formats in relation to health and healthcare; and (3) the ability to maintain health through self-management and working in partnerships with health providers (Liu et al., 2020). An accurate and consistent measurement of HL should integrate specific criteria that measure each element.
G20 policymakers should promote the definition of a clear HL global map based on shared indicators that measure the uptake of HL across countries to ensure that policies are targeted to the areas of greatest need.
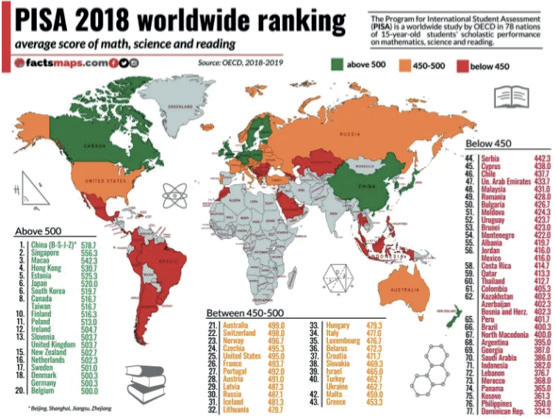
Figure 2. PISA 2018 Worldwide Ranking average score for mathematics, science and reading
(OECD, 2018)
Special attention should be given to particular countries, especially supporting data collection, taking into consideration the challenge that some countries and regions could face, as evidenced by Figure 2, which is a scientific literacy map.
PHASE 2
Making clear commitments: HL 2030 goals
Since building a culture of health awareness takes time and needs the collaboration of different stakeholders (from government institutions, academia, the private sector, civil society, media, etc.), shared clear commitments and goals on HL should be agreed upon for long-term standardized approaches.
HL 2030 goals should be promoted by G20 nations under the Alliance umbrella in order to set long-term common objectives and align international efforts. These should be identified in accordance with specific SDGs. Special attention should be dedicated to:
• SDG 3 Ensure healthy lives and promote well-being for all at all ages.
• SDG 4 Achieving inclusive and equitable access to education.
• SDG 17 Strengthen the means of implementation and revitalize the global partnership for sustainable development
Specific targets should be promoted within the HL 2030 goals to track their evolution and should be aligned with SDG 3, in order to measure their contribution in terms of promotion of health equality.
Clear institutional engagement: rebuilding trust between science, institutions and people
The pandemic has shown the importance of a strong relationship between governments and scientific communities. This must be based on mutual trust and clear communication to efficiently face challenges and mitigate anti-scientific narratives. The Lancet reports that the COVID-19 pandemic has highlighted HL as “an underestimated public health problem globally” (Paakari and Okan, 2020). Decision-makers have a responsibility to identify the HL needs of their populations and to invest in sustained public information campaigns as part of pandemic preparedness and response.
The findings we have outlined highlight the importance of specialized public institutions that support public health decisions with the help of health experts or advisors, scientists and university representatives. They can provide decision-makers with understandable and accurate scientific information, including disaggregated data and statistics, mitigating the risk of pseudoscientific intrusions into public policy and shaping the public debate with clear and accurate information boosting decision-makers’ critical role in promoting HL. A focused body could further review scientific evidence and papers, thereby identifying health priorities and investment (including innovation) and providing an efficient response to health needs through policymaking (Doubleday and Wilson, 2012; Morris et al., 2013; Nature, 2013, 2020; Reich, 2013; Cassel and Saunders, 2014; Gluckman, 2014; OECD, 2015; Senato, 2016; Kenny, 2017; Santillan-Garcia et al., 2020).
An example of a focused body is the European Commission’s Group of Scientific Advisors, which was formed by seven chief scientific advisors who were selected by an independent committee and appointed in their personal capacity to act independently and in the public interest. The mandate of the Group is to provide independent scientific advice to the European Commission and to make recommendations that will improve the interaction between policymaking and scientific advice (European Commission, n.d.). The advisors work together with the Scientific Advice for Policy by Academies (SAPEA) consortium, which is composed of over 100 European academic expertise of different science subjects, including medicine. Together with a secretariat in the Commission’s research and innovation department, the advisors and SAPEA are collectively known as the Scientific Advice Mechanism, which supports better and more scientifically validated policymaking.
Several countries have promoted such bodies with success, with examples to be found in France, Australia, Germany, Switzerland, Belgium, Norway and elsewhere (Kenny, 2017). There is still potential for these health-focused structures to be improved, allowing the HL challenge to be highlighted in all G20 countries so that resilience is strengthened, communities are able to innovate and future risks are prevented.
G20 leaders should promote the establishment of Health Advisory Boards at the highest level in each country to boost confidence and comprehension of health dynamics, progress and innovative solutions. The Alliance would also promote knowledge exchange and the adoption of good practices.
The role of the private sector and academia
The Alliance should promote a multi-stakeholder approach in order to build trust among diverse societal actors and enhance HL commitments. The private sector and academia could play an essential role in this by working together under the umbrella of the Alliance. The private sector could provide support so that financial and in-kind resources are mobilized, promoting partnerships with institutions to make effective investment that meets the current demand for HL. There is an unrecognized opportunity for the private sector to support the Alliance’s efforts, both to avoid the risk of public mistrust and to develop business opportunities. Despite the crucial role that life science companies have always played in producing and disseminating scientific knowledge, through the development of new technologies, services and products that have helped to enhance people’s health and well-being, the pandemic has highlighted the urgent need to strengthen public confidence in the functioning of this sector and to improve trust in scientific progress.
A strategic alliance is therefore necessary, starting with private sector biomedical innovations. This would include political institutions, thereby providing public involvement. Pharmaceutical companies shall be fully acknowledged as stable and trusted partners with the public, contributing through their commitment, investments and competencies to create shared value, and addressing health and broader social challenges such as HL in order to promote social well-being. Better rates of HL and a deeper understanding of the value and opportunity of innovative solutions on offer will contribute to overcoming access challenges and promoting equality. Clear commitments on HL goals are needed, taking into account the impact of industry contributions.
G20 leaders should launch a voluntary initiative based on the life sciences industry’s clear commitments to the achievement of HL goals in order to raise citizens’ awareness and undertake partnerships in support of SDGs (e.g. the Global Compact model).
The Alliance could also promote an ongoing dialogue and working groups between the academia and the private sector on issues of shared interest, including the improvement of access to open and free scientific information.
Providing open research data has the potential to improve research and to engage society, and also to contribute significantly to technology transfer and growth through innovation (European Commission, n.d.).
PHASE 3
Promoting shared platforms and contents for healthy habits
We are living in an era in which information sources have multiplied, as has the speed of their diffusion. Social media channels have radically changed these dynamics, democratizing the production of content which is no longer entrusted only to experts or mediators but their scientific value has been questioned (Eysenbach, 2008). Because of this, the ability of the individual to select contents on the basis of their validity, but also (and above all) their ability to critically assess them, and refute them if necessary, is crucial. The pandemic is teaching us that scientific information is a necessary but insufficient condition for a deep understanding of the dynamics of science and its solutions. The anti-scientific movements that have been reborn are tangible proof of this, and they risk undermining our global safety and our ability to respond to crises (Voss, 2018; McDougall, 2019).
The cause is not ignorance, or the absence of information (which would be easy to solve), but problems with the interpretation of information. This is the challenge of HL: to stimulate the production of information alongside critical thinking. A significant number of so-called conspiracy theorists are not ignorant people; on the contrary, they have often been educated to a high level. This makes the issue more complex and challenging. Those who are more educated, who have the ability to acquire information, can fall victim to confirmation bias when processing it at an individual level; in other words, they choose empirical data that confirm rather than disprove their beliefs but at the same time are unable to critically assess it. Starting from an initial assumption, the information they find will only further entrench their ideas. Being educated increases their self-esteem, and thus stimulating a debate is more difficult; even providing facts will not refute the initial assumption. Information is a tool that is used to increase confidence rather than knowledge (Drummond and Fischhoff, 2017). A related problem is that in many cases there is an unconscious inclination to check the veracity of information on the basis of its consistency with a view that is already held (Kunda, 1990). This overrides the value of evidence, and favours a search for connections with those in one’s own group.
Therefore, to counteract inadequate HL and the diffusion of disinformation, there is a need to work not just on accurate scientific facts and information, but also on helpful habits of thought, using the tools offered by the theory of bounded rationality, decision-making and choice architectures, and, chiefly, being aware of cognitive biases (Blumenthal-Barby and Krieger, 2015; Oxman and Garcia, 2020; Howell and Brossard, 2021).
For the next few years, it will therefore be necessary to investigate which are the most frequent biases that prevent the public from understanding today’s “knowledge society” and which are the most rational and critical cognitive tools through which this problem can be overcome, so that more effective (and ethically more sound) choices can be made in the interest of health and democracy (Flynn, 2012; Blummer and Kenton, 2014; Kahneman, 2021).
To promote fair and equal standards of HL, it will be crucial that G20 leaders promote the definition and sharing of accurate health content with the public, using social media awareness campaigns, gamification tools and apps to stimulate critical and healthy thinking habits; that is, the ability to apply the scientific method in all contexts.
PHASE 4
Promoting strategic cooperation for mutual learning and the attainment of collective objectives
International cooperation is a strategic tool that will ensure the achievement of equal standards of HL and progress towards required goals.
Through the Alliance, the G20 should promote the constitutions of specific regional working groups composed of institutions, academia, private sector, CSOs, communication experts and scientists in order to foster north-south and south-south partnerships, and to facilitate mutual learning between countries with varying levels of HL attainment. Ad hoc thematic sessions should be promoted with the participation of competent ministries in order to promote the HL 2030 Goals.
REFERENCES
Benziger CP, Roth GA, Moran AE (2016). The global burden of disease study and the preventable burden of NCD. Global Heart, 11(4):393-397
Berkman ND, et al. (2011). Health literacy interventions and outcomes: an updated systematic review. Evidence Report Technology Assessment, 199:1-941
Blumenthal-Barby JS, Krieger H. (2015). Cognitive biases and heuristics in medi al decision making: a critical review using a systematic search strategy. Medical Decision Making, 35(4): 539-557
Blummer B, Kenton JM (2014). Improving Student Information Search: A Metacognitive Approach. Oxford: Woodhead Publishing
Cassel CK, Saunders RS (2014). Engineering a better health care system: a report from the President’s Council of Advisors on Science and Technology. JAMA, 312(8):787-788
Coleman CA, et al. (2013). Health literacy practices and educational competencies for health professionals: a consensus study. Journal of Health Communication, 18, Suppl 1:82-102
Do BN (2020). Determinants of health literacy and its associations with health-related behaviors, depression among the older people with and without suspected COVID-19 symptoms: a multi-institutional study. Frontiers in Public Health, 8:581746
Doubleday R, Wilson J (2012). Beyond the great and good. Nature, 485:301-302
Drummond C, Fischhoff, B (2017). Individuals with greater science literacy and education have more polarized beliefs on controversial science topics. PNAS, 114(36):9587-9592
European Commission (n.d.a). The EU’s open science policy, https://ec.europa.eu/info/research-and-innovation/strategy/goals-research-and-innovation-policy/open-science/open-science-monitor_en, accessed 12 July 2021
European Commission (n.d.b). Group of chief scientific advisors, https://ec.europa.eu/info/research-and-innovation/strategy/support-policy-making/scientific-support-eu-policies/group-chief-scientific-advisors_en#about-the-advisors, accessed 12 July 2021
Eysenbach G (2008). Medicine 2.0: social networking, collaboration, participation, apomediation, and openness. Journal of Medical Internet Research, 10(3):e22
Fitzgerald DA, et al. (2020). Consequences of physical distancing emanating from the COVID-19 pandemic: an Australian perspective. Paediatric Respiratory Reviews, 35:25-30
Flynn J (2021). How to Improve Your Mind: Twenty Keys to Unlock the Modern World. Chichester, UK: Wiley-Blackwell
Gluckman P (2014). Policy: the art of science advice to government. Nature, 507(7491):163-165
Hoopman R, et al. (2009). Methodological challenges in quality of life research among Turkish and Moroccan ethnic minority cancer patients: translation, recruitment and ethical issues. Ethnicity and Health, 14(3):237-253
Howell EL, Brossard D (2021). (Mis)informed about what? What it means to be a science-literate citizen in a digital world. Proceedings of the National Academy of Sciences, 118(15):e1912436117
Institute of Medicine (2013). Health literacy around the world: part 1: health literacy efforts outside of the United States. In Health Literacy: Improving Health, Health Systems, and Health Policy around the World: Workshop Summary, by A Pleasant, 97-206. Washington, DC: National Academies Press
Ishikawa H, Yano E (2008). Patient health literacy and participation in the health-care process. Health Expectations, 11(2):113-122
Kahneman D (2021). Thinking Fast and Slow. London: Penguin
Kenny C, et al. (2017). Legislative science advice in Europe: the case for international comparative research. Palgrave Communications, 3(17030)
Kenny C, et al. (2017). Legislative science advice in Europe: the case for international comparative research. Palgrave Communications, 31(17030)
Kickbusch I, Maag D (2008). Health literacy. In International Encyclopedia of Public Health, Vol. 3. San Diego: Academic Press
Kickbusch I, Reddy KS (2016). Community matters: why outbreak responses need to integrate health promotion. Global Health Promotion, 23(1):75-78
Kobetz E, et al. (2009). Community-based participatory research in Little Haiti: challenges and lessons learned. Progress Community Health Partnership: Research, Education, and Action, 3(2):133-137
Kunda Z (1990). The case for motivated reasoning. Psychological Bulletin, 108(3):480-498
Liu C, et al. (2020). What is the meaning of health literacy? A systematic review and qualitative synthesis. Family Medicine and Community Health, 8(2)
McClintock HF, et al. (2017). Measurement of health literacy to advance global health research: a study based on demographic and health surveys in 14 sub-Saharan countries. The Lancet Global Health, 5, Suppl 1:S18
McDougall J (2019). Media literacy versus fake news: critical thinking, resilience, and civic engagement. Media Studies, 10:29-45
Mcqueen DV, Kickbusch I, Potvin L (2007). Health and modernity: the role of theory in health promotion. Internation Journal of Epidemiology, 34:226-228
Morris SA, et al. (2013). The PCAST report: impact and implications for the pharmaceutical industry. Clinical Pharmacology and Therapeutics, 94(3):300-302
Msaouel P, et al. (2014). Assessment of cognitive biases and biostatistics knowledge of medical residents: a multicenter, cross-sectional questionnaire study. Medical Education Online, 12(19):23646
Nature (2013). Look after the pennies, April:269
Nature (2020). Why Nature needs to cover politics now more than ever, October:169-170
Nazri HM (2019). Combatting pseudoscience: a science and health literacy workshop to improve scientific literacy in 16-year-old students in Malaysia. Malaysian Journal of Medical Sciences, 26(5):1-5
Nichols MD, Petzold AM (2021). A crisis of authority in scientific discourse. Cultural Studies of Science Education, 8(1):1-8
Nielsen-Bohlman L, Panzer A, Kindig D (2004). Health Literacy: A Prescription to End Confusion. Washington, DC: National Academies Press
Nutbeam, D (2000). Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promotion International, 15(3):259-267
OECD (Organisation for Economic Co-operation and Development) (2015). Scientific Advice for Policy Making. OECD Science, Technology and Industry Policy Papers, Paris
OECD (Organisation for Economic Co-operation and Development) (2017). G20/ OECD INFE Report on Adult Financial Literacy in G20 Countries. OECD
OECD (Organisation for Economic Co-operation and Development) (2018). PISA 2018 worldwide ranking: average score of mathematics, science and reading. FactsMaps, https://factsmaps.com/pisa-2018-worldwide-ranking-average-score-of-mathematics-science-reading/, accessed 12 July 2021
Oxman AD, Garcia LM (2020). Comparison of the Informed Health Choices Key Concepts Framework to other frameworks relevant to teaching and learning how to think critically about health claims and choices: a systematic review. F1000Research, 9:164
Paakkari L, Okan, O (2020). COVID-19: health literacy is an underestimated problem. Lancet Public Health, 5(5):e249e250
Peerson A, Saunders M (2009). Health literacy revisited: what do we mean and why does it matter? Health Promotion International, 24(3):285-296
PISA (Program for International Student Assessment) (2015). PISA 2015 Results: Volume 2: Policies and Practices for Successful Schools
PISA (Program for International Student Assessment) (2016). PISA 2015 Results: Excellence and Equity in Education. Paris: OECD
Pleasant A (2014). Advancing health literacy measurement: a pathway to better health and health system performance. Journal of Health Communication, 19(12):1481-1496.
Pleasant A, et al. (2015). Health literacy research and practice: a needed paradigm shift. Health Communication, 30(12):11761180
Reich ES (2013). Science’s go-to guy. Nature, 494:420-422
Santillan-Garcia A, et al. (2020). #CienciaenelParlamento: the need for a parliamentary office of science and technology advice. Health Gazette
Scherer LD, et al. (2021). Who is susceptible to online health misinformation? A test of four psychosocial hypotheses. Health Psychology, 40(4):274-284
Senato U (2016). Parlamenti e scienza: la valutazione dell’impatto scientifico e tecnologico. Servizio per la Qualità degli Atti Normativi
Siarova H, Sternadel D, Szőnyi E (2019). Research for CULT Committee: Science and Scientific Literacy as an Educational Challenge. Brussels: Policy Department for Structural and Cohesion Policies, European Parliament
Simonds SK (1974). Health education as social policy. Health Education Monographs, 2, Suppl 1:1-10
Solomon, M (2021). Trust: the need for public understanding of how science works. Hastings Center Report, 51, Suppl 1:S36-S39
Sørensen K, et al. (2012). Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health, 12: 80
Sørensen PJM, et al. (2015). Health literacy in Europe: comparative results of the European Health Literacy Survey (HLSEU). European Journal of Public Health, 25(6):1053-1058
Thomas GP, Durant, JR (1987). Why should we promote the public understanding of science? In Scientific Literacy Papers, ed. M Shortland, 1-14. Oxford: Rewley House
Voss, J (2018). Who learns from collaborative digital projects? Cultivating critical consciousness and metacognition to democratize digital literacy learning. Composition Studies, 46(1):57-80
WHO (World Health Organization) (2017). Policy Brief 4: Health Literacy, 9th Global Conference on Health Promotion. Shanghai: World Health Organization
Zarocostas J (2020). How to fight an infodemic. The Lancet, 395(10225):676